Fill Out Your Maryland Confidential Morbidity Report Template
Fill Out Your Maryland Confidential Morbidity Report Template
Do's:
Don'ts:
This form is not limited to physicians. Other health care providers can also complete and submit it. It is essential for anyone involved in patient care to understand their role in reporting.
While the report does focus on certain conditions, it encompasses a variety of morbidity data. This includes chronic diseases and other health conditions that may impact public health.
Submitting the Maryland Confidential Morbidity Report is a legal requirement for certain conditions. Health care providers must comply to ensure the health department can monitor and manage public health effectively.
Confidentiality is a cornerstone of this reporting system. The information collected is protected under state and federal laws, ensuring that patient identities remain confidential.
While the report is sent to local health departments, it contributes to a larger state database. This data helps in tracking trends and outbreaks across Maryland.
The Maryland Confidential Morbidity Report is regularly updated to reflect current public health needs. Providers should always use the latest version to ensure compliance and accuracy.
Failure to submit required reports can lead to legal repercussions for health care providers. It is crucial to prioritize reporting to avoid potential penalties and ensure community safety.
Maryland State Compliance Application - Ensure to note down the social security number and EIN where necessary.
How to Write a Land Purchase Agreement - In the event of property damage before settlement, the buyer has the option to terminate the contract.
Understanding the intricacies of your financial obligations is vital, and a solid foundation can be established by reviewing a detailed loan agreement, which highlights terms associated with borrowing and repayment.
Maryland State Tax Forms - If applicable, provide details on state or federal rehabilitation tax credits.
Once the Maryland Confidential Morbidity Report form is completed, it must be submitted to your local health department. Ensure all information is accurate and thorough, as this report plays a crucial role in public health monitoring and response. After submission, your local health department may reach out for any additional details needed regarding the case.
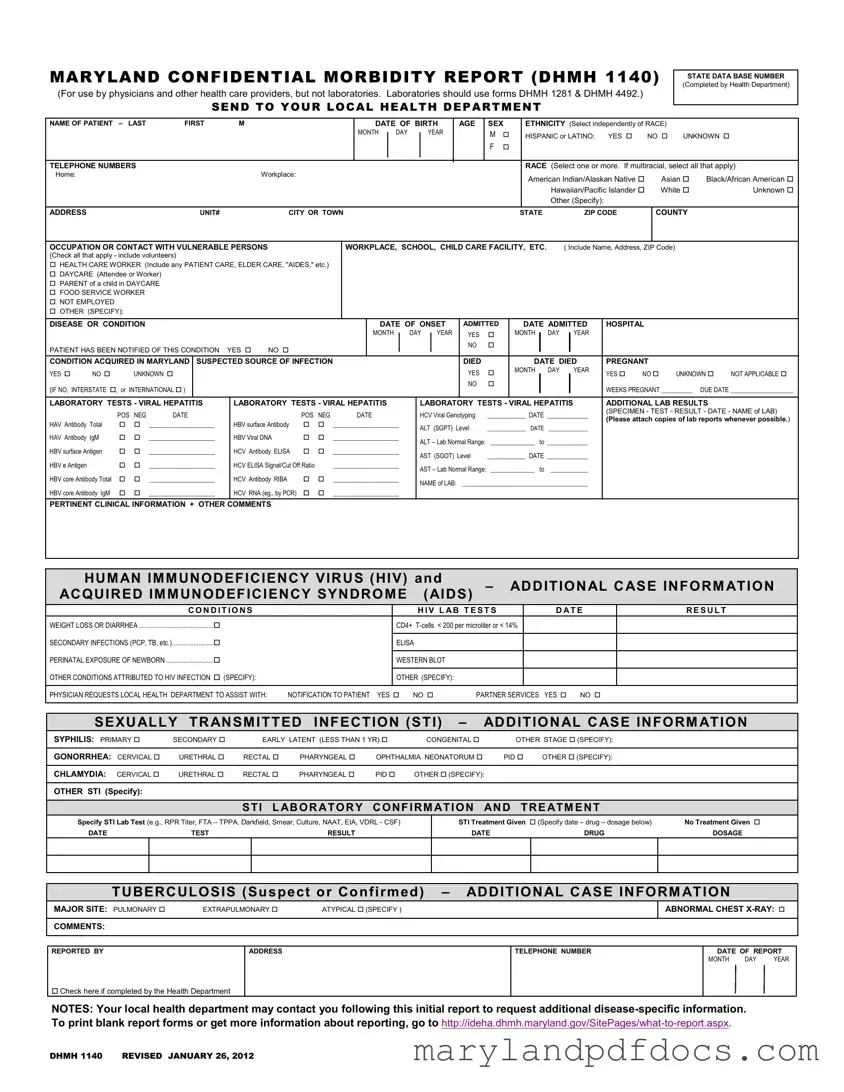
MARYLAND CONFIDENTIAL MORBIDITY REPORT (DHMH 1140)
(For use by physicians and other health care providers, but not laboratories. Laboratories should use forms DHMH 1281 & DHMH 4492.)
SEND TO YOUR LOCAL HEALTH DEPARTMENT
STATE DATA BASE NUMBER (Completed by Health Department)
NAME OF PATIENT |
– LAST |
FIRST |
|
M |
|
|
|
|
|
|
DATE OF BIRTH |
|
AGE |
SEX |
|
ETHNICITY (Select independently of RACE) |
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
MONTH |
|
DAY |
|
|
YEAR |
|
|
M |
|
|
HISPANIC or LATINO: |
YES |
|
NO |
UNKNOWN |
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TELEPHONE NUMBERS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RACE (Select one or more. If multiracial, select all that apply) |
|||||||||||||||||
Home: |
|
|
|
|
|
|
|
Workplace: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
American Indian/Alaskan Native |
|
Asian |
Black/African American |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hawaiian/Pacific Islander |
|
White |
|
Unknown |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Other (Specify): |
|
|
|
|
|
|
|
|||
ADDRESS |
|
|
|
|
UNIT# |
|
|
CITY OR TOWN |
|
|
|
|
|
|
|
|
|
|
|
STATE |
|
|
ZIP CODE |
|
|
COUNTY |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
OCCUPATION OR CONTACT WITH VULNERABLE PERSONS |
|
|
|
WORKPLACE, SCHOOL, CHILD CARE FACILITY, ETC. |
|
( Include Name, Address, ZIP Code) |
|
|
|
|||||||||||||||||||||||||||||||||
(Check all that apply - include volunteers) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
HEALTH CARE WORKER (Include any PATIENT CARE, ELDER CARE, "AIDES," etc.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
DAYCARE (Attendee or Worker) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
PARENT of a child in DAYCARE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
FOOD SERVICE WORKER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
NOT EMPLOYED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OTHER (SPECIFY): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
DISEASE OR CONDITION |
|
|
|
|
|
|
|
|
|
|
DATE OF ONSET |
ADMITTED |
|
|
DATE ADMITTED |
|
HOSPITAL |
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MONTH |
|
|
DAY |
|
YEAR |
YES |
|
|
MONTH |
|
|
DAY |
|
YEAR |
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
PATIENT HAS BEEN NOTIFIED OF THIS CONDITION |
YES |
NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
CONDITION ACQUIRED IN MARYLAND |
SUSPECTED SOURCE OF INFECTION |
|
|
|
|
|
|
|
|
|
|
|
|
|
DIED |
|
|
|
|
DATE DIED |
|
PREGNANT |
|
|
|
|||||||||||||||||
YES |
NO |
|
UNKNOWN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
|
|
MONTH |
DAY |
|
YEAR |
|
YES |
NO |
UNKNOWN |
NOT APPLICABLE |
||||||||
(IF NO, INTERSTATE , or INTERNATIONAL ) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NO |
|
|
|
|
|
|
|
|
|
|
|
WEEKS PREGNANT __________ |
DUE DATE ____________________ |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LABORATORY TESTS - VIRAL HEPATITIS |
|
LABORATORY TESTS - VIRAL HEPATITIS |
|
|
|
|
LABORATORY TESTS - VIRAL HEPATITIS |
|
ADDITIONAL LAB RESULTS |
|
||||||||||||||||||||||||||||||||
|
|
POS |
NEG |
DATE |
|
|
|
POS |
NEG |
|
|
DATE |
|
|
|
|
HCV Viral Genotyping |
____________ |
DATE _____________ |
|
(SPECIMEN - TEST - RESULT - DATE - NAME of LAB) |
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
(Please attach copies of lab reports whenever possible.) |
||||||||||||||||||||||||||||||
HAV Antibody Total |
|
|
_____________________ |
|
HBV surface Antibody |
|
|
_____________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
ALT (SGPT) Level |
______________ |
DATE |
______________ |
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
HAV Antibody IgM |
|
|
_____________________ |
|
HBV Viral DNA |
|
|
_____________________ |
|
|
|
ALT – Lab Normal Range: |
______________ to _____________ |
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
HBV surface Antigen |
|
|
_____________________ |
|
HCV Antibody ELISA |
|
|
_____________________ |
|
|
|
AST (SGOT) Level |
____________ |
DATE _____________ |
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
HBV e Antigen |
|
|
|
_____________________ |
|
HCV ELISA Signal/Cut Off Ratio |
|
_____________________ |
|
|
|
AST – Lab Normal Range: ______________ to |
____________ |
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
HBV core Antibody Total |
|
|
_____________________ |
|
HCV Antibody RIBA |
|
|
_____________________ |
|
|
|
NAME of LAB: |
________________________________________ |
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
HBV core Antibody IgM |
|
|
_____________________ |
|
HCV RNA (eg., by PCR) |
|
|
_____________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
PERTINENT CLINICAL INFORMATION + OTHER COMMENTS
|
HUMAN IMMUNODEFICIENCY VIRUS (HIV) and |
– |
ADDITIONAL CASE INFORMATION |
||||
|
ACQUIRED IMMUNODEFICIENCY SYNDROME |
(AIDS) |
|||||
|
CON D IT IO NS |
|
H IV L AB T EST S |
|
D AT E |
RESULT |
|
|
WEIGHT LOSS OR DIARRHEA ............................................. |
CD4+ |
|
|
|||
|
SECONDARY INFECTIONS (PCP, TB, etc.)......................... |
|
|
|
|
|
|
|
ELISA |
|
|
|
|
|
|
|
PERINATAL EXPOSURE OF NEWBORN ............................. |
|
|
|
|
|
|
|
WESTERN BLOT |
|
|
|
|
||
|
OTHER CONDITIONS ATTRIBUTED TO HIV INFECTION (SPECIFY): |
|
|
|
|
|
|
|
OTHER (SPECIFY): |
|
|
|
|
||
PHYSICIAN REQUESTS LOCAL HEALTH DEPARTMENT TO ASSIST WITH: NOTIFICATION TO PATIENT YES NO PARTNER SERVICES YES NO
SEXUALLY TRANSMITTED INFECTION (STI) – |
ADDITIONAL CASE INFORMATION |
|||||
SYPHILIS: PRIMARY |
SECONDARY |
EARLY LATENT (LESS THAN 1 YR) |
CONGENITAL |
OTHER STAGE (SPECIFY): |
||
|
|
|
|
|
|
|
GONORRHEA: CERVICAL |
URETHRAL |
RECTAL |
PHARYNGEAL |
OPHTHALMIA NEONATORUM |
PID OTHER (SPECIFY): |
|
|
|
|
|
|
|
|
CHLAMYDIA: CERVICAL |
URETHRAL |
RECTAL |
PHARYNGEAL |
PID |
OTHER (SPECIFY): |
|
|
|
|
|
|
|
|
OTHER STI (Specify): |
|
|
|
|
|
|
STI LABORATORY CONFIRMATION AND TREATMENT
Specify STI Lab Test (e.g., RPR Titer, FTA – TPPA, Darkfield, Smear, Culture, NAAT, EIA, VDRL - CSF)
DATE |
TEST |
RESULT |
STI Treatment Given (Specify date – drug – dosage below) |
No Treatment Given |
|
DATE |
DRUG |
DOSAGE |
TUBERCULOSIS (Suspect or Confirmed) – ADDITIONAL CASE INFORMATION
MAJOR SITE: PULMONARY |
EXTRAPULMONARY |
ATYPICAL (SPECIFY ) |
ABNORMAL CHEST
COMMENTS:
REPORTED BY
ADDRESS
TELEPHONE NUMBER
DATE OF REPORT
MONTH DAY YEAR
Check here if completed by the Health Department
NOTES: Your local health department may contact you following this initial report to request additional
DHMH 1140 REVISED JANUARY 26, 2012
Incomplete Patient Information: Failing to provide all necessary details about the patient, such as their full name, date of birth, and contact information, can lead to delays in processing the report.
Incorrect Ethnicity and Race Selection: Selecting ethnicity and race incorrectly or not understanding the distinction between the two can result in inaccurate demographic data.
Missing Disease or Condition Details: Omitting the specific disease or condition and its date of onset can hinder public health responses and tracking efforts.
Inaccurate Laboratory Test Results: Reporting lab results incorrectly or neglecting to include necessary laboratory tests can compromise the quality of the data collected.
Failure to Notify Patient: Not indicating whether the patient has been notified of their condition can lead to miscommunication and potential legal issues.
Omitting Follow-Up Information: Leaving out critical follow-up details, such as treatment given or additional comments, can prevent appropriate health interventions.
What is the purpose of the Maryland Confidential Morbidity Report form?
The Maryland Confidential Morbidity Report form is designed for healthcare providers to report specific diseases and conditions to local health departments. This report helps public health officials track and manage disease outbreaks, ensuring that appropriate measures are taken to protect community health. It is important for physicians and other healthcare providers to fill out this form accurately to facilitate timely responses to public health concerns.
Who is required to complete this form?
This form is primarily for use by physicians and healthcare providers. It's important to note that laboratories should not use this form; instead, they should utilize forms DHMH 1281 and DHMH 4492 for reporting. Healthcare providers, including those working in hospitals, clinics, and other medical settings, are responsible for submitting the report when they diagnose a reportable condition.
What information is needed to complete the form?
To complete the Maryland Confidential Morbidity Report form, healthcare providers must provide various details about the patient, including their name, date of birth, sex, ethnicity, and race. Additionally, information regarding the disease or condition, date of onset, hospital admission details, and laboratory test results must be included. It’s also essential to indicate if the patient has been notified of their condition and whether the condition was acquired in Maryland.
How is patient confidentiality maintained when using this form?
Patient confidentiality is a top priority when using the Maryland Confidential Morbidity Report form. The form is designed to be confidential, and the information collected is used solely for public health purposes. Local health departments are responsible for safeguarding this information and ensuring that it is only accessible to authorized personnel. Providers should take care to submit the form securely and avoid sharing any identifiable patient information outside of the reporting process.
What should I do if I need more information about reporting?
If you require additional information about how to report or need blank report forms, you can visit the Maryland Department of Health's website at http://ideha.dhmh.maryland.gov/SitePages/what-to-report.aspx. This site provides resources and guidance on the reporting process, ensuring that healthcare providers have the necessary tools to comply with reporting requirements effectively.